Backed by MORE than 60 Published RESEARCH ARTICLES
Contact us for more infoPublished Scientific and Research Articles
Osteoarthritis in Obese Individuals
Clinical context
Obesity and osteoarthritis both reduce mobility. Obesity is a risk factor for osteoarthritis. Osteoarthritis causes people who are overweight or obese to exercise less and possibly eat more than appropriate for their low activity levels.
Women with osteoarthritis have slightly reduced lean mass relative to body weight. Therefore, losing and maintaining weight is difficult for people with osteoarthritis. Many individuals may have complicating factors for cardiovascular disease, which could mean bariatric surgery is not an option even if otherwise eligible. A new solution for weight problems in osteoarthritis is therefore needed.
192
Patients
16 wks.
Total duration
+12%
Weight lost
60%
Symptom relief
Study methodology
One hundred and ninety-two patients were treated with very low-calorie diets (415 to 540 kcal/d) or low-calorie (810 kcal/d) liquid diets for eight weeks, then a 1,200 kcal/d diet (which included two portions of formula diets) for 8 weeks, combined with weekly group education, for a total of 17 sessions.
Results
More than 12% of initial body weight was lost in both groups, with 60% having a good symptom response in both groups.
Eight of 96 dropped out of the very low-calorie diet group, 6 of 96 dropped out of the low-calorie diet group.
Thus, for this group of individuals there appears to be no advantage in terms of weight loss from using a very low-calorie diet over a low-calorie diet.
Implications of the results
A good method of weight loss and maintenance for obese individuals with osteoarthritis is sufficient weight loss to reduce symptoms, especially pain, improve mobility and maintain or improve body composition (fat loss, lean tissue retention), improve cardiovascular risk and improve or maintain vitamin D status and bone health (during and after weight loss remodelling, which typically results in mineral loss).
Thus, the weight loss approach with the formula diet programmes described in this paper has been shown to deliver a package of health benefits rather than simply weight loss and its maintenance.
Documented benefits package
- 1
The evidence relating to obesity and osteoarthritis is reviewed in: Bliddad H, Leeds AR, Christensen R. Osteoarthritis and weight loss. Hard facts, hypotheses and horizons: a scoping review. Obesity Reviews 2014; 15 (7):578-86. Doi: 10.1111/obr.12173. Epub 2014 Apr 22.
- 2
Christensen P, Bliddal H, Riecke BF, Leeds AR, Astrup A, Christensen R. Comparison of low-energy and very low-energy diets in sedentary obese individuals: a pragmatic randomized controlled trial in clinical obesity, first published online: 21 MAR 2011 | DOI: 10.1111/j.1758-8111.2011.00006.x.
- 3
Riecke BF, Christensen R, Christensen P, Leeds AR, Boesen M, Lohmander LS, Astrup A, Bliddal H. Comparing two low-calorie diets for the treatment of symptoms in obese patients with knee osteoarthritis: a randomised clinical trial. Osteoarthritis and Cartilage 2010; 10/1016/j.joca.
Obstructive Sleep Apnoea in Obese Individuals
Clinical context
Sleep apnoea can originate from problems in the part of the brain that controls breathing. Obstructive sleep apnoea (OSA) is caused by a blockage in airflow, due to excess fat in the tissue near where air normally passes and a failure of the surrounding muscles.
Obstructive sleep apnoea is said to occur when airflow through the mouth and nose stops for more than 10 seconds at least 30 times in 7 hours of sleep. Some surveys indicate that one in four people with diabetes mellitus may have OSA, others that four in five obese people with diabetes have it. There are no precise data on the rate of OSA for the general population; perhaps one in 25 or more. Obstructive sleep apnoea may be a factor in raising blood pressure. Those who have suffered but survived a heart attack normally reveal they had sleep apnoea before the event. Sleep apnoea is therefore a condition best avoided.
63
Patients
9 wks.
VLCD phase
-12 kg
Weight lost
17 u.
AHI improvement
Does obstructive sleep apnoea really matter?
OSA causes sleep interrupted by pauses in breathing during sleep. But it can also cause poor-quality rest and lead the sufferer to fall asleep at work. Quality of life can be seriously affected by daily fatigue, poor concentration, irritability, forgetfulness, morning headaches and sexual dysfunction.
What causes sleep apnoea?
Factors linked to OSA include variations in the size and shape of the upper airway, excess weight, and genetic history of the condition. Scientific studies indicate that the airways in obese individuals are thicker, which obstructs airflow.
This article is important because
It is the first randomised controlled analysis using VLCD in severe and moderate sleep apnoea.
It provides high-quality evidence on the outcome of VLCD diets in weight loss and, consequently, improving OSA symptoms in male patients.
After 9 weeks, those in the control group moved on to follow the 9-week diet. All patients were offered a maintenance programme with ongoing support, as well as the option to use a formula product to maintain weight for 1 year.
Results after 1 year
After 1 year, apnoea-hypopnoea indices improved by 17 units, while body weight was 12 kg less than at the start. 30 of 63 subjects no longer require CPAP and 6 of 63 achieved full remission. Those who lost the most weight or had the highest sleep apnoea index benefited the most.
- 1
Johansson K, et al. Longer term effects of very low energy diet on obstructive sleep apnoea in cohort derived from randomised controlled trial prospective observational follow-up study. BMJ 2011: 342:d3017 doi: 10.1136/bmj.d3017.
- 2
Foster DG, Borradiale KE, Sanders MH, et al. Randomised study on the effect of Weight loss in obstructive sleep apnea among obese patients with type 2 diabetes. Arch Int Med 2009; 169 (17): 1619-1626.
- 3
Tuomilehto HPI, Seppä JM, Partinen MM et al. Lifestyle intervention with weight reduction: first line treatment in mild obstructive sleep apnoea. Am J Respir Crit Care Med 2009; 179: 320-327.
- 4
Johansson K, Neovius M, Lagerro YT, Harlid R, Rossner S, Granath F, Hemmingsson E. Effect of a very low energy diet on obese individuals with severe and moderate obstructive sleep apnoea: a randomised controlled trial. BMJ 2009; 339: b4609 doi: 10.1136/bmj.
Weight maintenance after loss with a VLCD or LCD formula
Context
There is a belief that weight regain occurs quickly after using a VLCD or LCD formula, probably reflecting the failure of nutritionists to implement an effective maintenance strategy. How to maintain a low-energy diet and a more physically demanding level of activity are topics that have been under investigation for years.
3,017
Participants
20
Studies
-12.3 kg
VLCD/LCD average
27
Analysis arms
Meta-analysis methodology
This meta-analysis was designed to evaluate the effects of anti-obesity medications (sibutramine and orlistat), diets or exercise on weight maintenance after a VLCD or LCD. It consisted of a systematic review of English-language articles using MEDLINE, the Cochrane Controlled Trial Register and EMBASE, from 1981 to February 2013, with expert physicians in the field contracted. Included studies were randomised controlled analyses specifically evaluating weight maintenance strategies after undergoing a VLCD or LCD.
20 studies, 27 arms and a total of 3,017 participants were included: anti-obesity drugs (3 arms, n=658), meal replacement (4 arms, n=322), high-protein diets (6 arms, n=865), dietary supplements (6 arms, n=261), other diets (3 arms, n=564) and exercise (5 arms, n=347).
During the VLCD/LCD period, the average weight lost was 12.3 kg (mean duration: 8 weeks, range 3–16).
Results compared with placebo or control
Compared with placebo or control, the intervention significantly changed weight loss maintenance:
Anti-obesity medications: 3.5 kg less (95% CI -5.5, -1.5; mean duration 18 months, range 12–36).
Meal replacement: 3.9 kg less (95% CI -5.0, -2.8; mean duration 12 months, range 10–26).
High-protein diets: 1.5 kg less (95% CI -2.1, -0.8; mean duration 5 months, range 3–12).
In contrast to the above results, the differences between the following groups were not significant:
Exercise: 0.8 kg (95% CI -2.8, 1.2; mean duration 10 months, range 6–12).
Dietary supplements: 0.0 kg (95% CI -1.4, 1.4; mean duration 3 months, range 3–14).
Consequently, anti-obesity medications, meal replacements and high-protein diets were associated with improved weight maintenance after using a VLCD or LCD.
Conclusion
Since sibutramine has been withdrawn in Europe, the only current interventions with improvements in weight maintenance after a VLCD or LCD are orlistat, conventional meal replacement with a formula diet and the use of a high-protein diet.
Original article
(Article in English)
 Not available
Not available - 1
Effects of anti-obesity drugs, diet and exercise on weight loss maintenance after a very low-calorie diet or low-calorie diet: a systematic review and meta-analysis of randomised controlled trials. Johansson K, Neovius M, Hemmingsson E. Am J Clin Nutr 2013 published online 30 October 2013.
Transition to primary care
Main outcome
A care package including initial weight loss with a Cambridge Weight Plan programme, followed by food reintroduction and weight maintenance (Counterweight Programme) yielded a reduction of more than 15 kg after 1 year in one third of participants.
91
Participants
BMI >40
Clinical profile
-15 kg
In 1 year
1/3
Achieved it
Study description
The study, presented in February 2013 in The British Journal of General Practice by Professor Mike Lean and colleagues from the University of Glasgow and the Counterweight programme team, describes the outcomes of the weight loss intervention in 91 people with BMI >40 living in rural areas or small towns in Scotland.
Severe obesity is rapidly increasing in Scotland: 6% of men and 11% of women are subjects with a BMI greater than 35, and for those over 55 years of age, results indicate 3% of men and 5% of women with BMI above 40. Potentially eligible for surgery, some of these cases with BMI exceeding 40 are ineligible for that treatment under those circumstances, as they still require a loss of between 15 and 20 kg for their metabolism to function adequately.
Formula diet programmes, offering a nutrient-rich diet, achieve a smaller energy intake deficit than conventional diets. These higher rates of weight reduction have been shown to be safe, and mass losses yielded a notable result in older individuals with osteoarthritis (Christensen et al 2011).
Participants in these trials were individuals with a long diabetes-free history; therefore, there is now a need to conduct a similar study in those with type 2 diabetes. Strategies to reduce dropout still need to be refined, as do methods for maintaining weight after 1 year.
Two evaluated interventions
In the weight loss trial in individuals with osteoarthritis, participants were distributed into 2 random groups to take part in 2 active programmes.
Programme 1
Daily use of a formula product as a meal substitute to help reduce caloric intake to 400 kcal/d after a 15 kg loss, along with close monitoring and the use of an 800 kcal/d liquid diet if weight were to increase by more than 2 kg.
Programme 2
A 5-week opportunity for an 800 kcal/d liquid diet every 4 months. This randomised trial will determine whether it is possible to maintain weight and which of the 2 interventions produces the best results.
- 1
Weight loss and maintenance with formula diet now feasible in primary care. Lean M, Brosnahan N, McLoone P, McCombie L, Bell-Higgs A, Ross H, Mackenzie M, Grieve E, Finer N, Reckless J, Haslam D, Sloan B, Morrison D. Feasibility and indicative results from a 12-month low-energy-liquid-diet treatment and maintenance programme for severe obesity. Br J Gen Pract 2013; DOI: 10.3399/bjgp13X663073.
Psoriasis
Clinical context
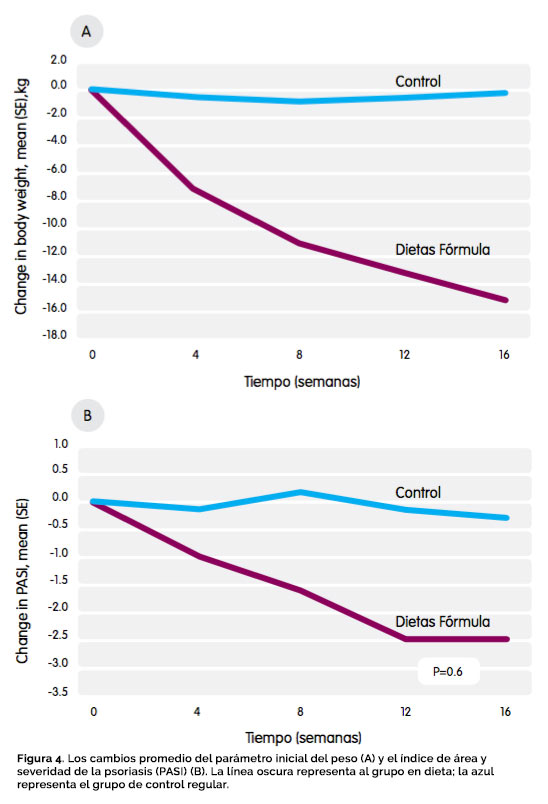
Psoriasis is a recurrent chronic inflammatory skin condition characterised by patches of thick, scaly redness, which vary depending on circumstances. It is worth noting that genetic and environmental factors play an important role in the development of psoriasis. It is associated with obesity, as it is not observed in very slim individuals, and may be more severe when mass increases. Until the publication of the work described here, there was no medical evidence that weight reduction was beneficial.
60
Patients
800–1,000
kcal/day CWP
-15.4 kg
More than control
DLQI
Index improved
Methodology and results
60 patients presenting with obesity and psoriasis were allocated to regular weight management or a Cambridge Weight Plan diet of 800–1,000 kcal/d, followed by a 1,200 kcal/d diet for 8 weeks in preparation for a maintenance programme.
The diet-treated group lost 15.4 kg more than the group on regular management. The Dermatology Life Quality Index (DLQI) improved significantly after the diet compared with the regular management group, and the Psoriasis Area and Severity Index (PASI) showed a major improvement.
Results will be presented at the end of 2014.

- 1
Effect of Weight Loss on the severity of Psoriasis. Jensen, P., et al. JAMA Dermatol doi: 10.1001/jamadermatol.2013.722 (published on line 29 May 2013).
- 2
Miller IM, Ellervik C, Yazdanyar S, et al. (2013) Meta-analysis of psoriasis, cardiovascular disease, and associated risk factors. J Am Acad Dermatol 69: 1014-24.
- 3
Jensen P, Zachariae C, Christensen R et al. (2014) Effect of Weight Loss on the Cardiovascular Risk Profile of Obese Patients with Psoriasis. Acta Derm Venereol doi: 10.2340/00015555-1824.
- 4
Geiker N R W, Jensen P, Zachariae C et al. (2014) Effect of weight loss on the severity of psoriasis: one year follow-up. T5: S41.04. Obesity Reviews 15(S2): 170-1. doi: 10.1111/obr.12151/
Osteoarthritis — Additional articles
Want to learn more about these articles? Click the button to download.

Improved nutritional status and bone health after diet-induced weight loss in sedentary osteoarthritis patients: a prospective cohort study
(Article in English)
P Christensen, EM Bartels, BF Riecke, H Bliddal, AR Leeds, A Astrup, K Winther and R Christensen. European Journal of Clinical Nutrition (2012) 66, 504–509; doi:10.1038/ejcn.2011.201; published online 21 December 2011.

Effects of an intensive weight loss program on knee joint loading in obese adults with knee osteoarthritis
(Article in English)
P Christensen, EM Bartels, BF Riecke, H Bliddal, AR Leeds, A Astrup, K Winther and R Christensen. European Journal of Clinical Nutrition (2012) 66, 504–509; doi:10.1038/ejcn.2011.201; published online 21 December 2011.

Comparing two low-energy diets for the treatment of knee osteoarthritis symptoms in obese patients: a pragmatic randomized clinical trial
(Article in English)
P Christensen, EM Bartels, BF Riecke, H Bliddal, AR Leeds, A Astrup, K Winther and R Christensen. European Journal of Clinical Nutrition (2012) 66, 504–509; doi:10.1038/ejcn.2011.201; published online 21 December 2011.

Comparison of a low-energy diet and a very low-energy diet in sedentary obese individuals: a pragmatic randomized controlled trial
(Article in English)
P Christensen, EM Bartels, BF Riecke, H Bliddal, AR Leeds, A Astrup, K Winther and R Christensen. European Journal of Clinical Nutrition (2012) 66, 504–509; doi:10.1038/ejcn.2011.201; published online 21 December 2011.
Sleep apnoea — Additional articles
Want to learn more about these articles? Click the button to download.

Effect of a very low energy diet on moderate and severe obstructive sleep apnoea in obese men: a randomised controlled trial
(Article in English)
Kari Johansson, PhD student, Martin Neovius, postdoctoral research fellow, Ylva Trolle Lagerros, physician, Richard Harlid, physician, Stephan Rössner, professor, Fredrik Granath, statistican, Erik Hemmingsson, postdoctoral research fellow. BMJ 2009;339:b4609 doi:10.1136/bmj.b4609.

Does medically induced weight loss improve obstructive sleep apnoea in the obese: review of randomized trials
(Article in English)
P Christensen, EM Bartels, BF Riecke, H Bliddal, AR Leeds, A Astrup, K Winther and R Christensen. European Journal of Clinical Nutrition (2012) 66, 504–509; doi:10.1038/ejcn.2011.201; published online 21 December 2011.

Effect of a very low-energy diet on moderate and severe obstructive sleep apnoea: case reports
(Article in English)
P Christensen, EM Bartels, BF Riecke, H Bliddal, AR Leeds, A Astrup, K Winther and R Christensen. European Journal of Clinical Nutrition (2012) 66, 504–509; doi:10.1038/ejcn.2011.201; published online 21 December 2011.
Diabetes — Additional articles
Want to learn more about these articles? Click the button to download.

Using a low energy formula diet in obese patients with long-standing insulin-treated Type 2 diabetes produces significantly greater weight loss, improvement in glucose control and insulin reductions compared to gold standard clinical care over a 12 week period
(Article in English)
AC Brown, S Taheri, A Dornhorst, N Kapoor, B McGowan, AR Leeds and G Frost.

VLED and formula LED in the management of type 2 diabetes: defining the clinical need and research requirements
(Article in English)
Lean, M. Clinical Obesity 2011; 1(1): 41-49. DOI: 10.1111/j.1758-8111.2010.00007.x.

A systematic review of waist-to-height ratio as a screening tool for the prediction of cardiovascular disease and diabetes: 0·5 could be a suitable global boundary value
(Article in English)
Lucy M. Browning, Shiun Dong Hsieh and Margaret Ashwell. Nutrition Research Reviews (2010), 23, 247–269. doi:10.1017/S0954422410000144.

National Diabetes Institute Malaysia Diabetes Asia 2010 Conference. Sleep Apnoea, Obesity and Diabetes – Mechanisms and Treatment
(Article in English)
Anthony R Leeds. University of Surrey UK, University of Copenhagen Denmark, and Cambridge Weight Plan. October 6th to 10th 2010, Kuching, Sarawak, Malaysia.
Trials — Additional articles
Want to learn more about these articles? Click the button to download.

Comparison of a low-energy diet and a very low-energy diet in sedentary obese individuals: a pragmatic randomized controlled trial
(Article in English)
P. Christensen, H. Bliddal, B. F. Riecke, A. R. Leeds, A. Astrup and R. Christensen. Clinical Obesity © 2011 International Association for the Study of Obesity. doi: 10.1111/j.1758-8111.2011.00006.x.

A weight loss formula diet improved vitamin D status in obese, older individuals: a cohort study exploring safety in a randomised controlled trial
(Article in English)
Christensen P, Bartels EM, Riecke BF, Bliddal H, Leeds AR, Astrup A, Winther K, Christensen R. Obesity Reviews 2011; 12 (Suppl 1) 59-60 (T5:OS3.4).

Improved nutritional status after a weight loss formula diet: a cohort study exploring safety in a randomised controlled trial
(Article in English)
Christensen P, Riecke BF, Bliddal H, Leeds AR, Astrup A, Winther K, Christensen R. Obesity Reviews 2010; 11 (suppl 1): 247 (T3:PO.81).
Rheumatology · Surgery · Psoriasis
Want to learn more about these articles? Click the button to download.

Rheumatology
Osteoarthritis – a role for weight management in rheumatology practice: an update
(Article in English)
H. Bliddal, P. Christensen, B. F. Riecke, J. Aaboe, R. Frederiksen, E. Bartels, R. Christensen. © 2011 The Authors Clinical Obesity © 2011 International Association for the Study of Obesity. DOI: 10.1111/j.1758-8111.2010.00008.x.

Surgery
Ergem: effects of roux-en-y gastric bypass surgery on energy metabolism
(Article in English)
Schmidt JB, Gregersen NT, Pedersen S, Hansen DL, Worm D, Madsbad S, Astrup A and Sjödin A. © 2011 The Authors. Obesity Reviews 12 (Suppl. 1) (2011) 63–279.

Psoriasis
Weight loss and skin manifestations in obese patients with psoriasis – a controlled randomized cross-over study
(Article in English)
Larsson LK, Geiker NRW, Jensen P, Zachariae C, Astrup A and Skov L. © 2011 The Authors. Obesity Reviews 12 (Suppl. 1) (2011) 63–279.